2.8.4
Bone blocks
Bone blocks Bone blocks Bone blocks Bone blocks Bone blocks Bone blocks Bone blocks
A widely-spread method of compensation for alveolar bone volume is transfer of bone blocks. In this, we most frequently implant fragments taken from the mental area 2.8.4-1C or retromolar area (external oblique line).
There are several methods of extraction of donor fragments: piezoelectric surgery, Lindeman drills, disc and tangential saws, et. al.), with special conditions of an atermic and atraumatic mode of preparation. Following the transfer to the target position, a fragment is fixed with micro-screws for bones 2.8.4-1D. Stability and immobility of the transplanted block is essential to successful surgery.
The issue with this method is that the donor bone fragments are mostly cortical, and they are steady in form, but poorly vascularized. Thus, in the course of the transplantation and integration part of the bone volume is lost, sometimes considerable.
The main surgical problem here is not working with the bone proper, but immobilization of soft tissues and covering the site of transplantation without expressed tension of the tissues.
2.8.4-1A At first, mucus-periosteal flaps are reclined in the defect area, and the amount to be recovered is determined.
2.8.4-1B Extraction of a fragment from the mental area should be performed quickly, yet accurately!
2.8.4-1C A donor fragment is transferred to the defect site. During the removal of the fragment, holes are made for the fixing screws.
2.8.4-1D The fragment is firmly fixed with mini-screws.
2.8.4-1E All cavities between the fragment and the site are filled with CollapAn-N.
2.8.4-1F After sutures are applied, the whole area is treated with Solcoseryl-Dental ointment.
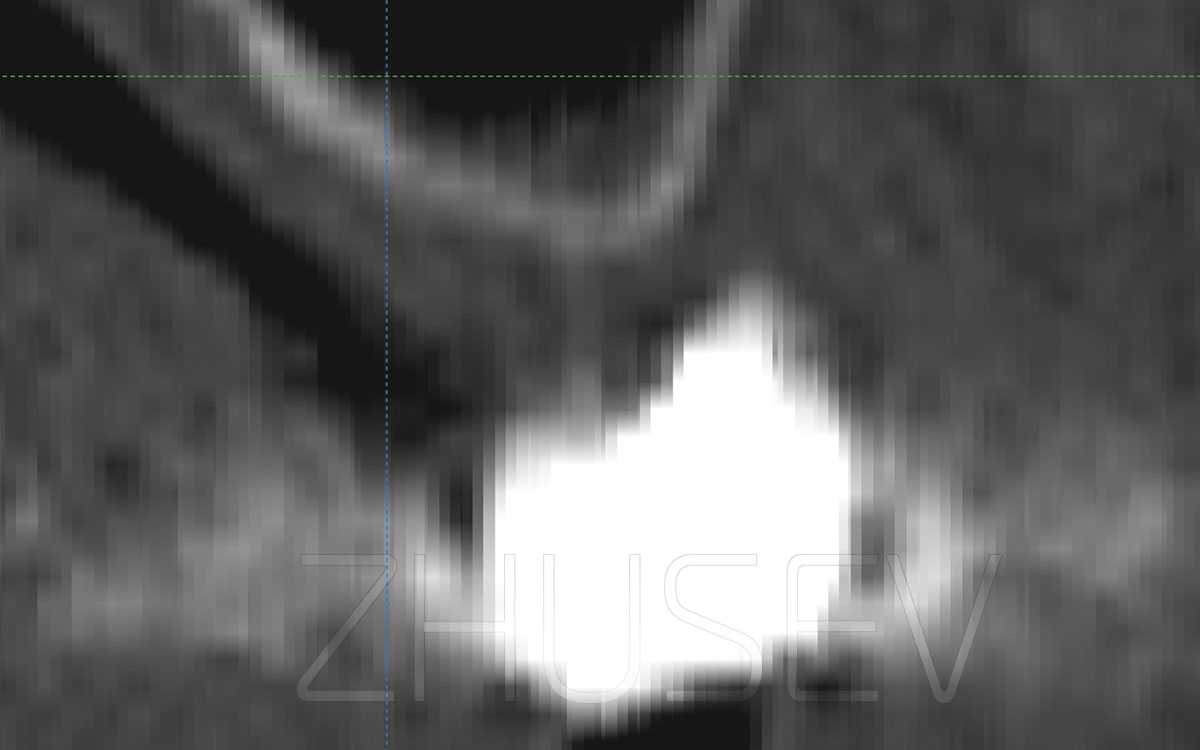
2.8.4-1G Reference X-ray is made 12 weeks after the transplantation of the bone block.
2.8.4-1H View inside mouth cavity 3 ½ weeks after the transplantation of the bone block.
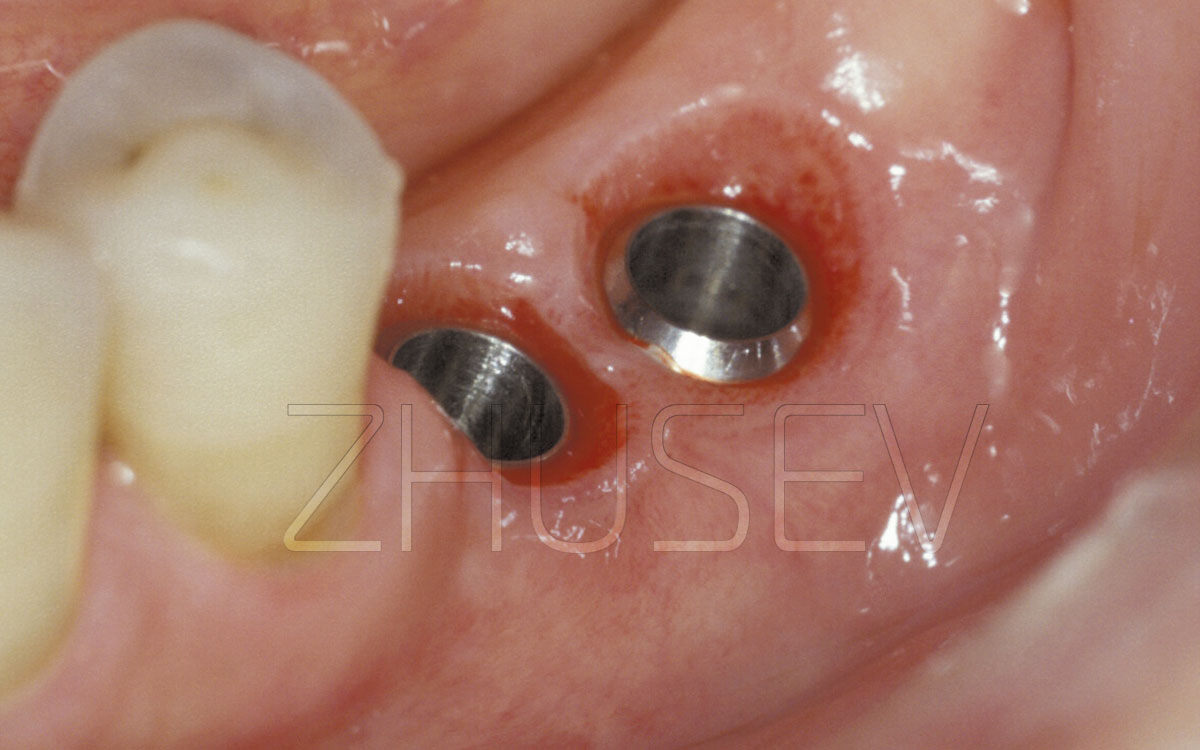
2.8.4-1I Mucoperiosteal flaps are reclined. The head of the fixing screw lies on the transplanted bone block, and this means the fragment’s atrophy is minimal.
2.8.4-1J The fixing screw is removed. The bone block is homogeneous with the recipient jaw.
2.8.4-1K The newly formed bone is prepared for receiving the implant. The bone tissue is dense and well-vascularized.
The appearance and topography of a bone defect are decisive in choosing a method of supplementation surgery. If the defect resulted from orthodontic procedures and the gap narrows down from the palatal and vestibular sides to its middle, splitting is preferable.
In my opinion, the most reasonable place to extract a bone block from is the mental (mandibular) area. This practically excludes any risk of paresthesia for the lower alveolar nerve. Mind that the block should be formed at least 3-4 mm below the top of the roots. Defining the size of the block and its extraction should be performed only after the placement location has been prepared!
If the defect appeared during traumatic extraction of a tooth, or after serious inflammation or loss of implant, and as a result the vestibular wall is nearly lost, but the palatal wall is available, it will be better to transplant a bone block.
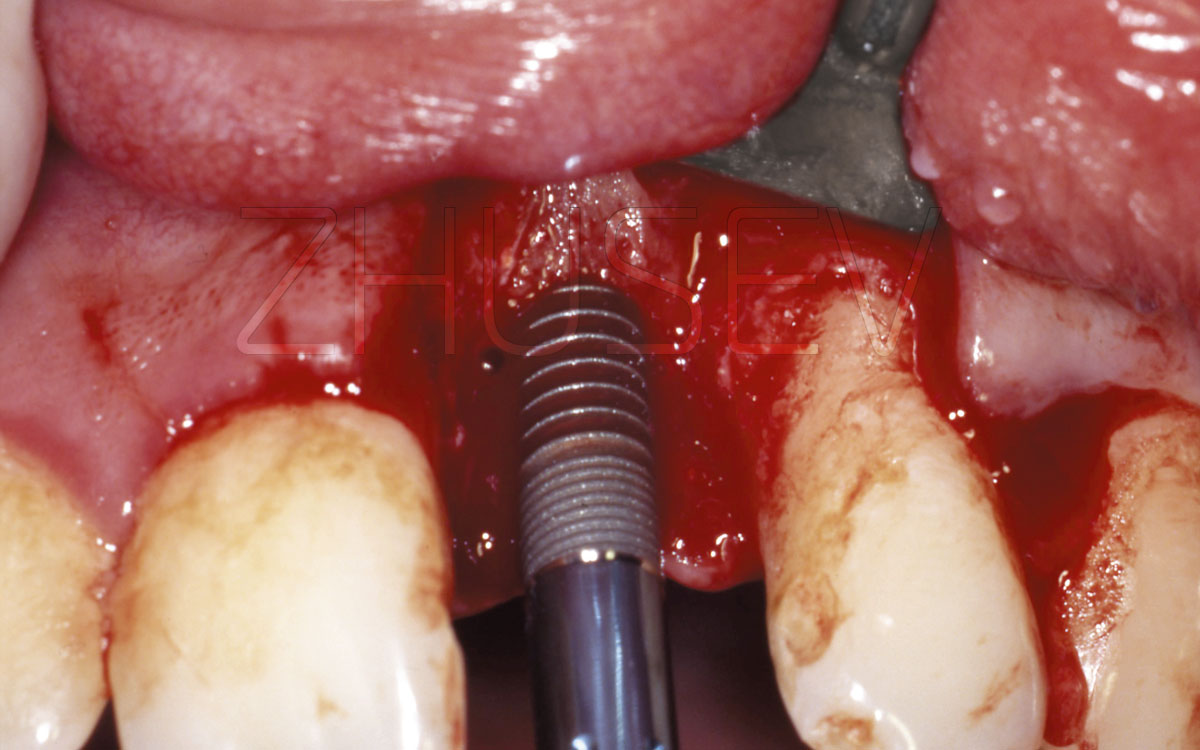
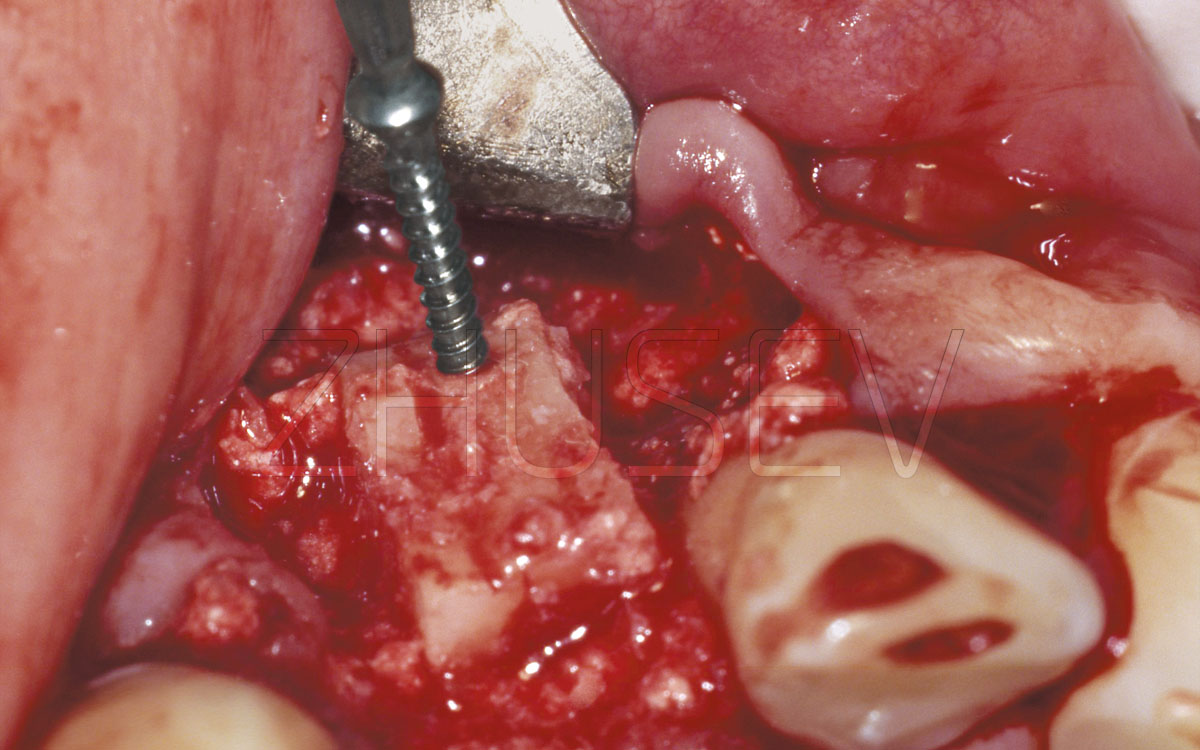
2.8.4-1L Installation of a CONMET implant. Blood wetting of the implant surface here is excellent.
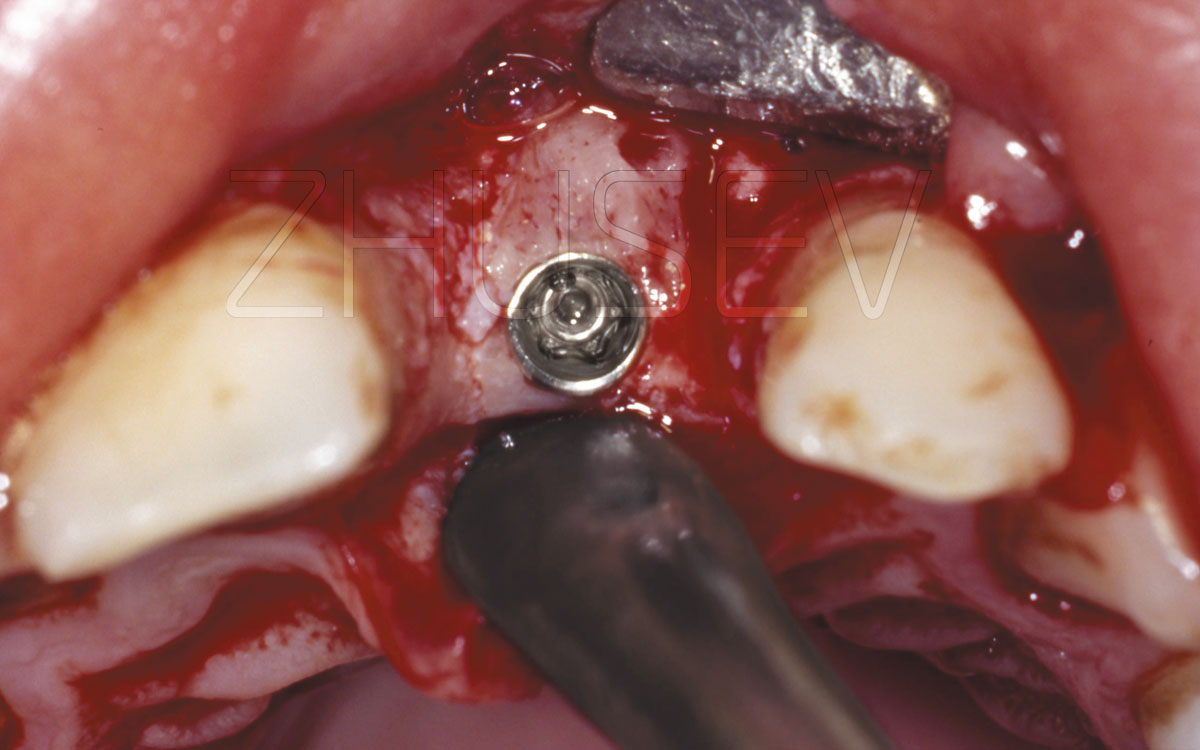
2.8.4-1M Note that the implant is placed at the border between the transplanted bone and the palatal plate.
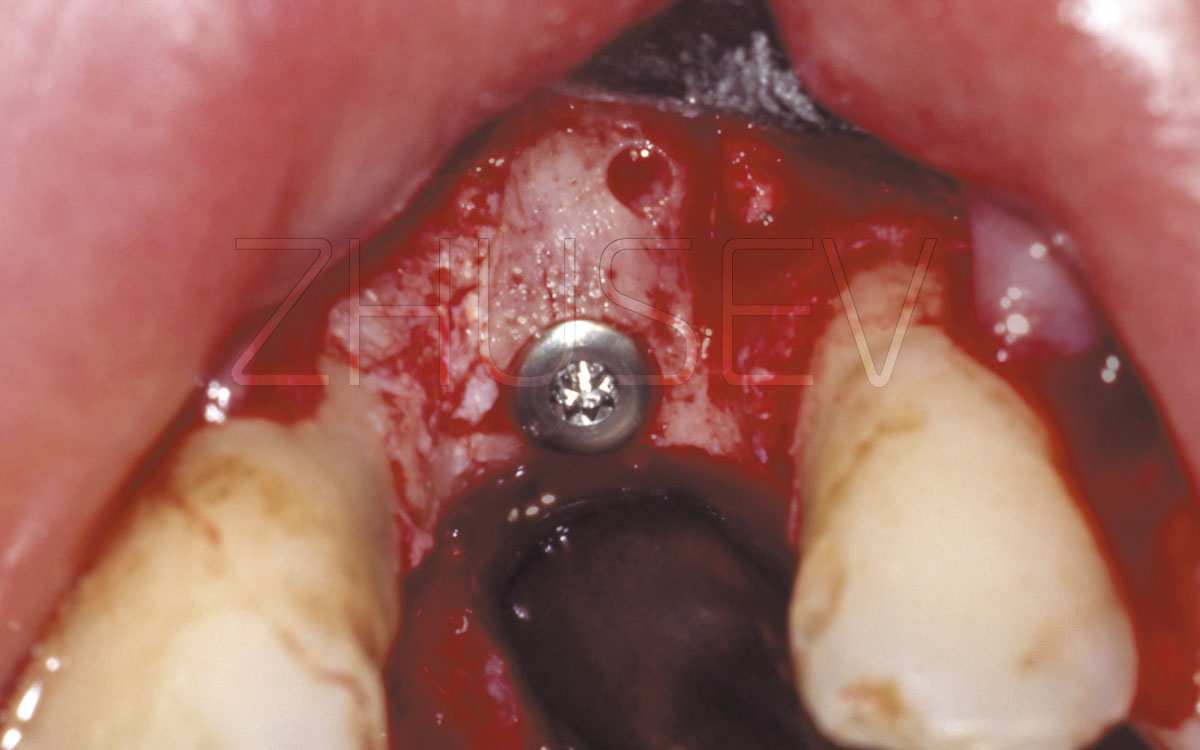
2.8.4-1N
The implant is fully installed in the bone. A cover screw is turned in.
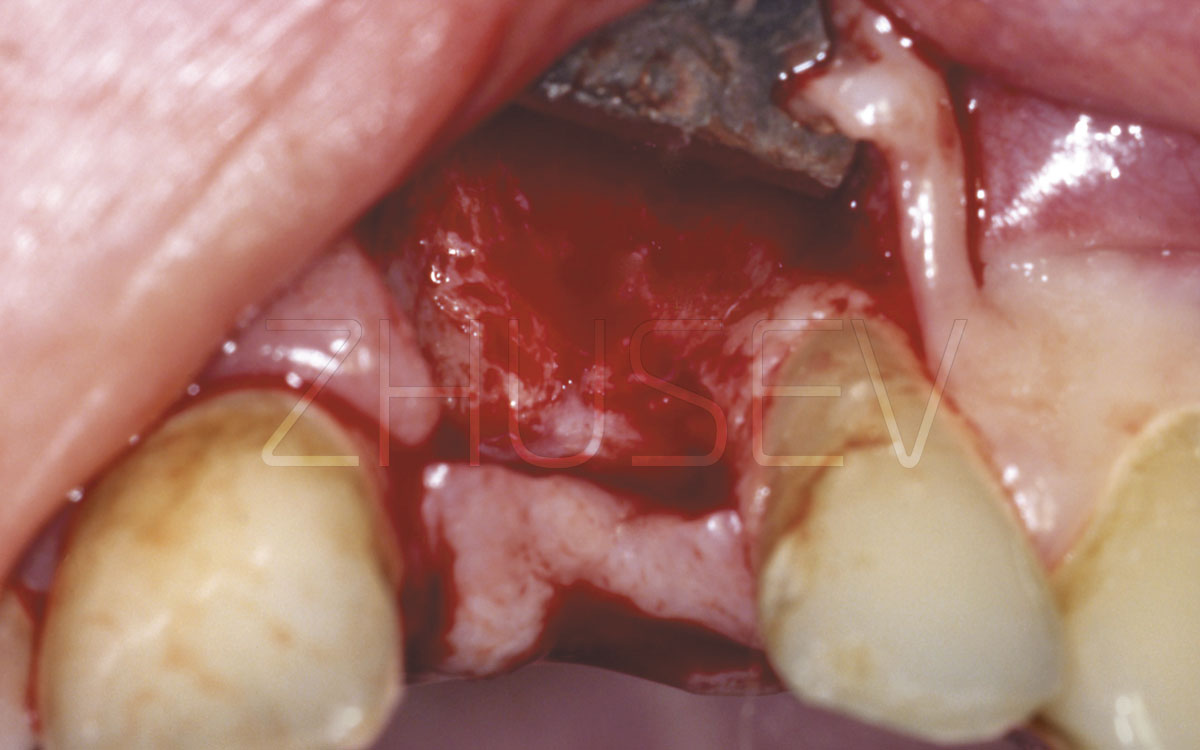
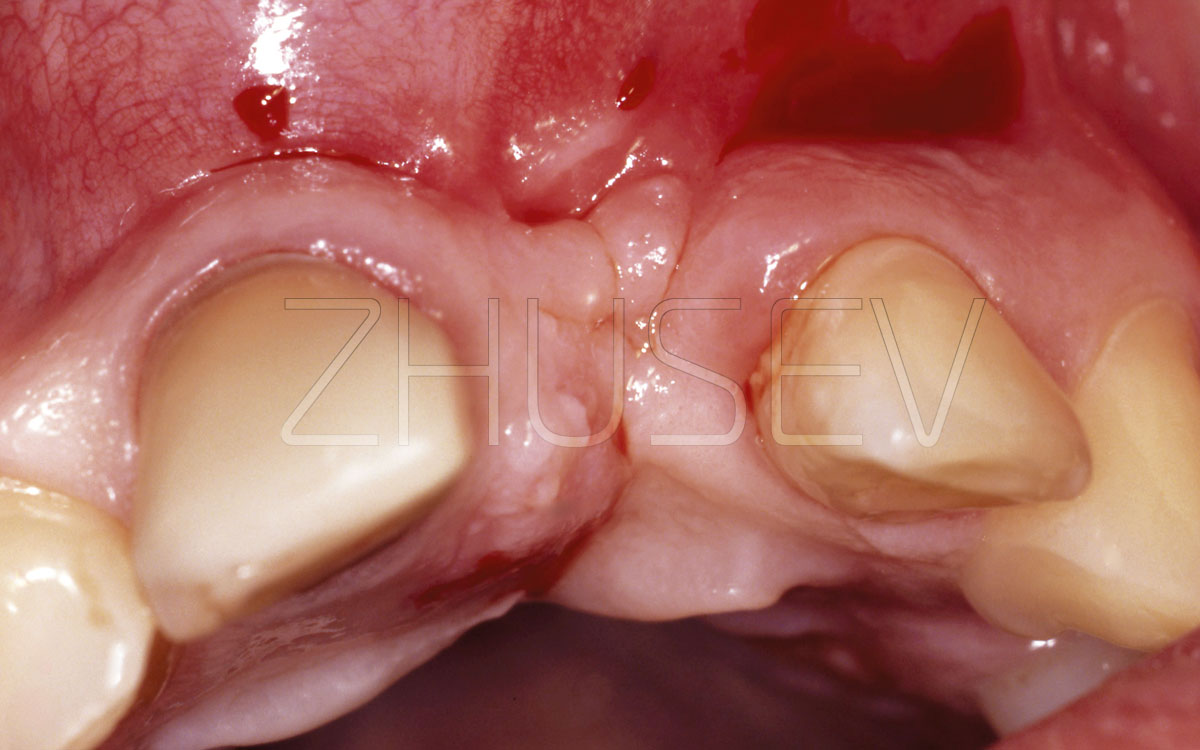
2.8.4-2A
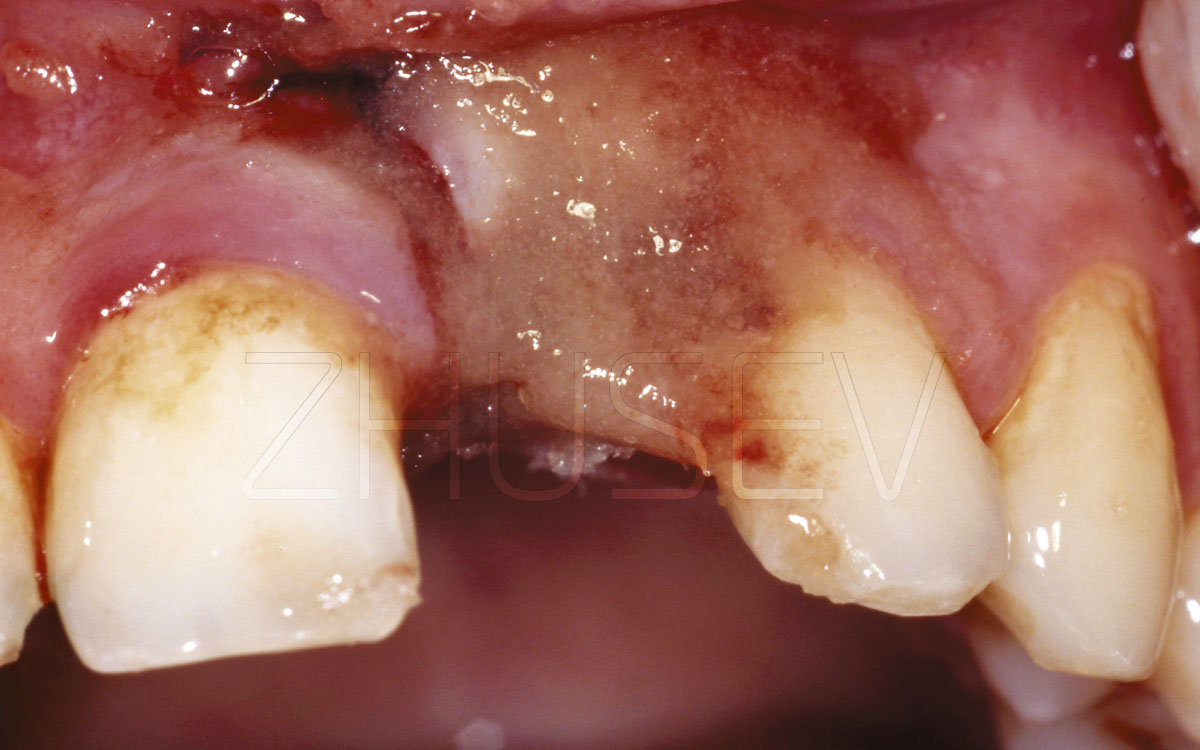
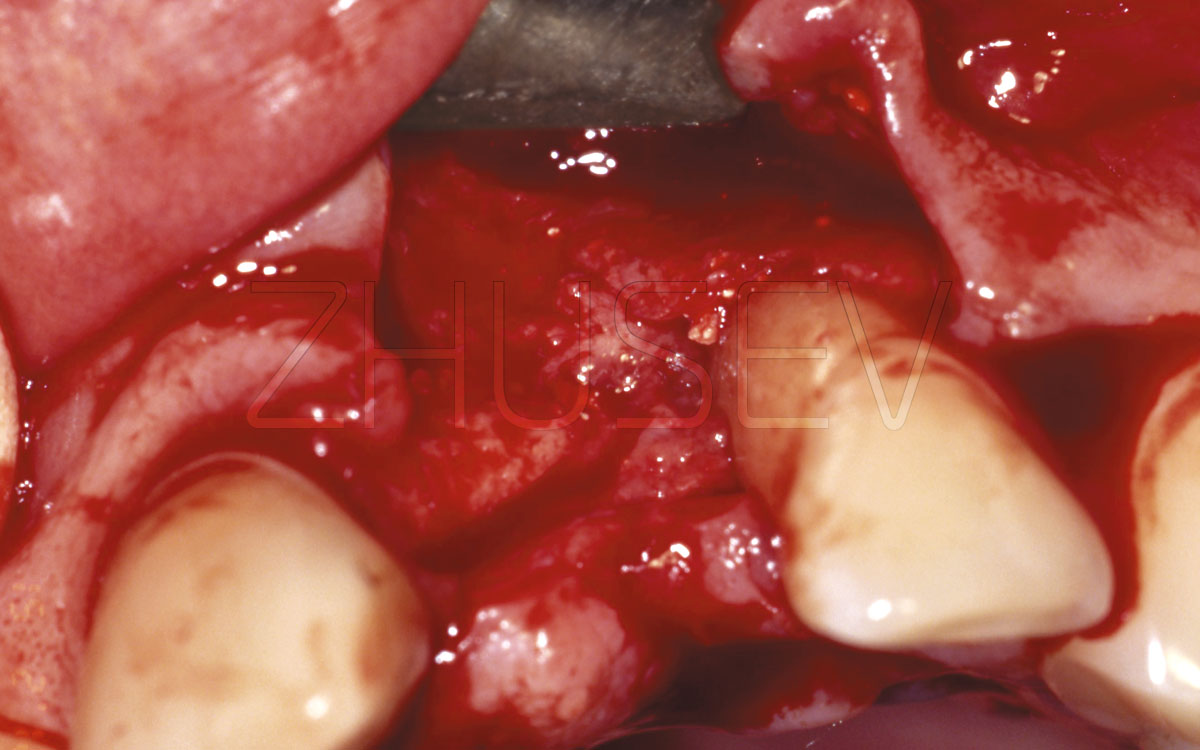
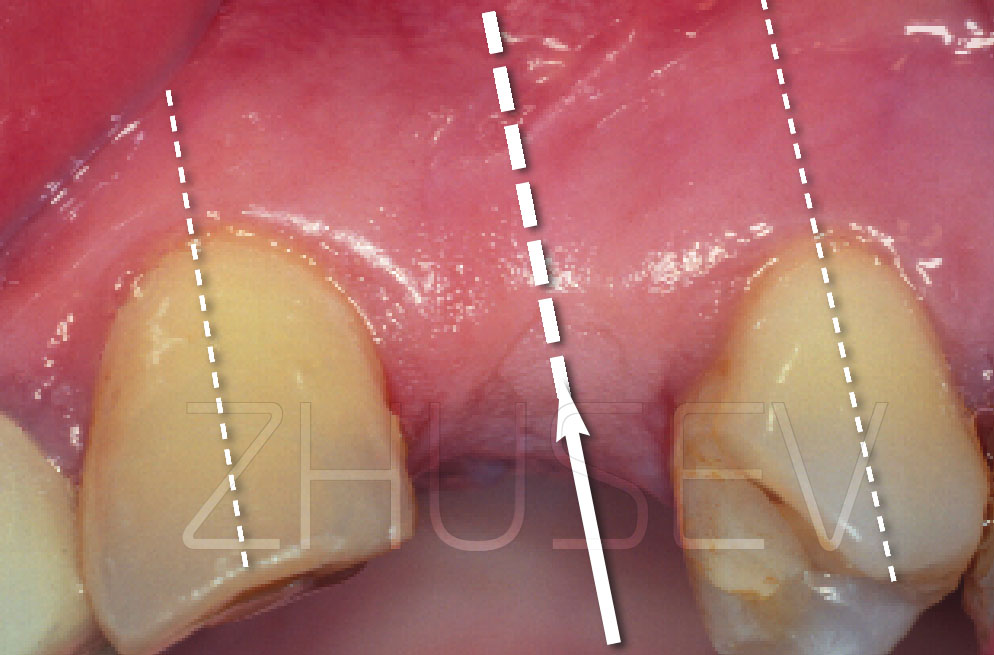
This is the patient’s first visit to our clinic, after osteoplastic correction of the defect has failed twice. You can see significant cicatrical changes of the mucosa.
2.8.4-2B
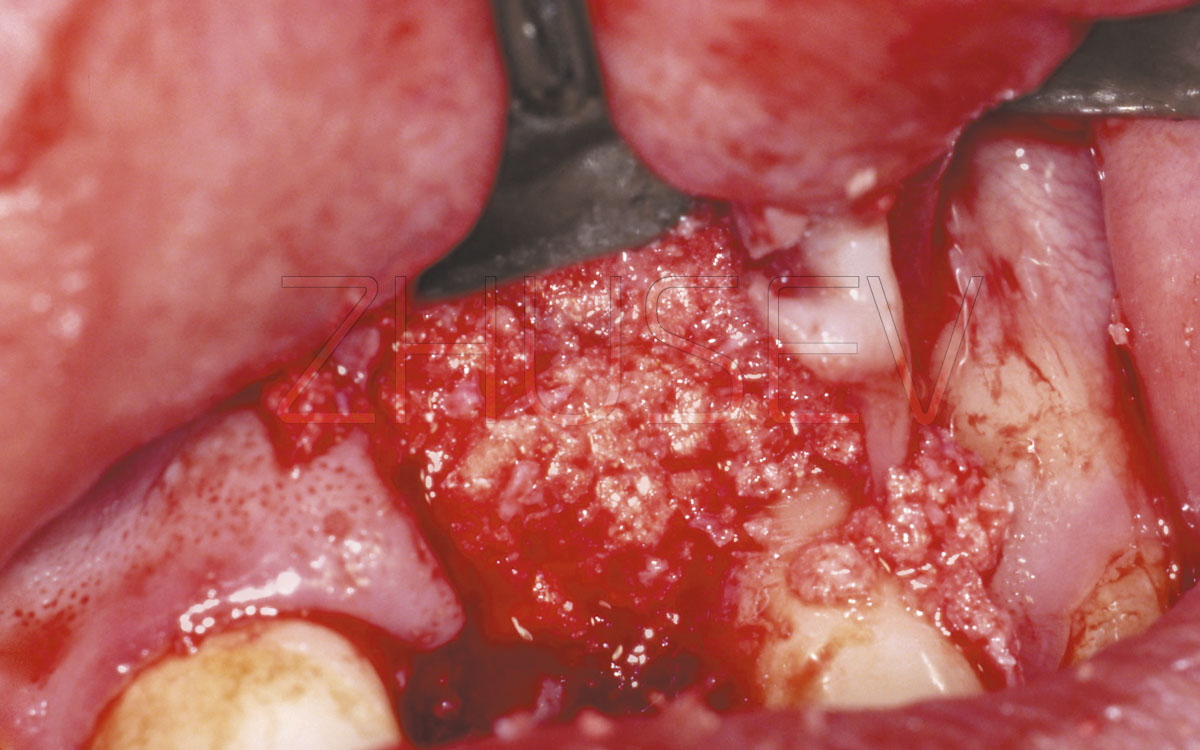
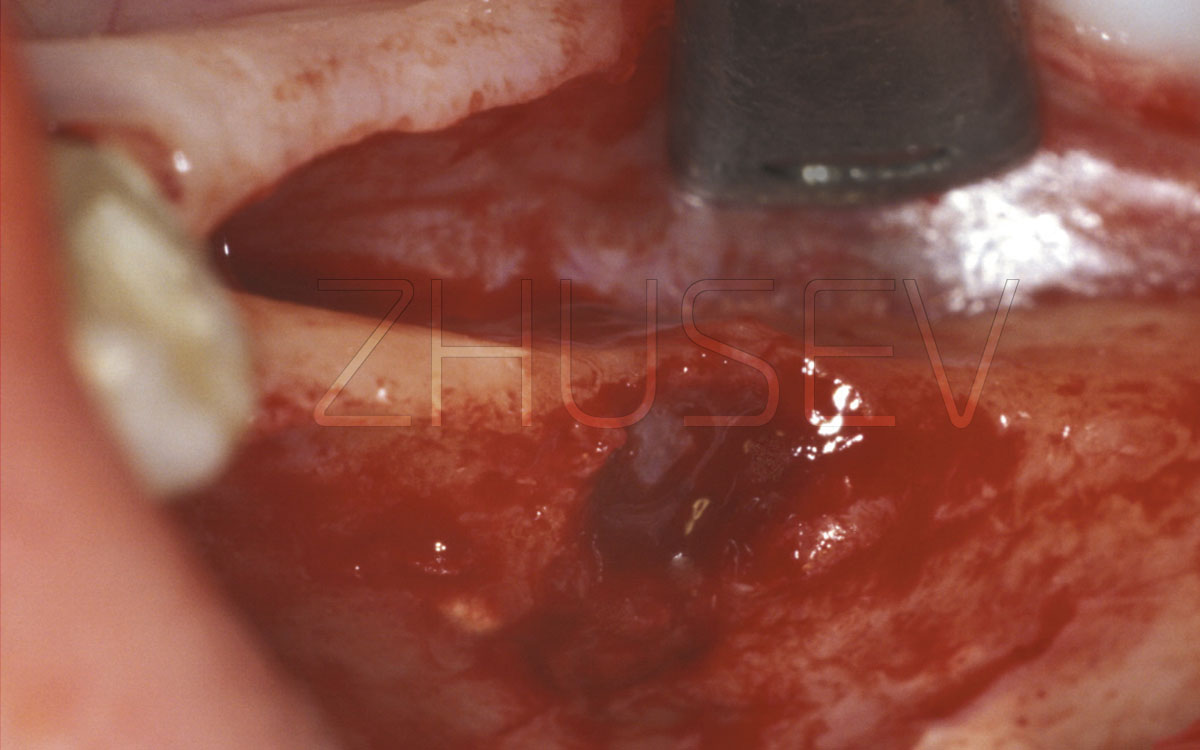
Opening the mucoperiosteal flaps, we find a great bone defect and a deep bone pocket at tooth 22, filled with granulation tissue.
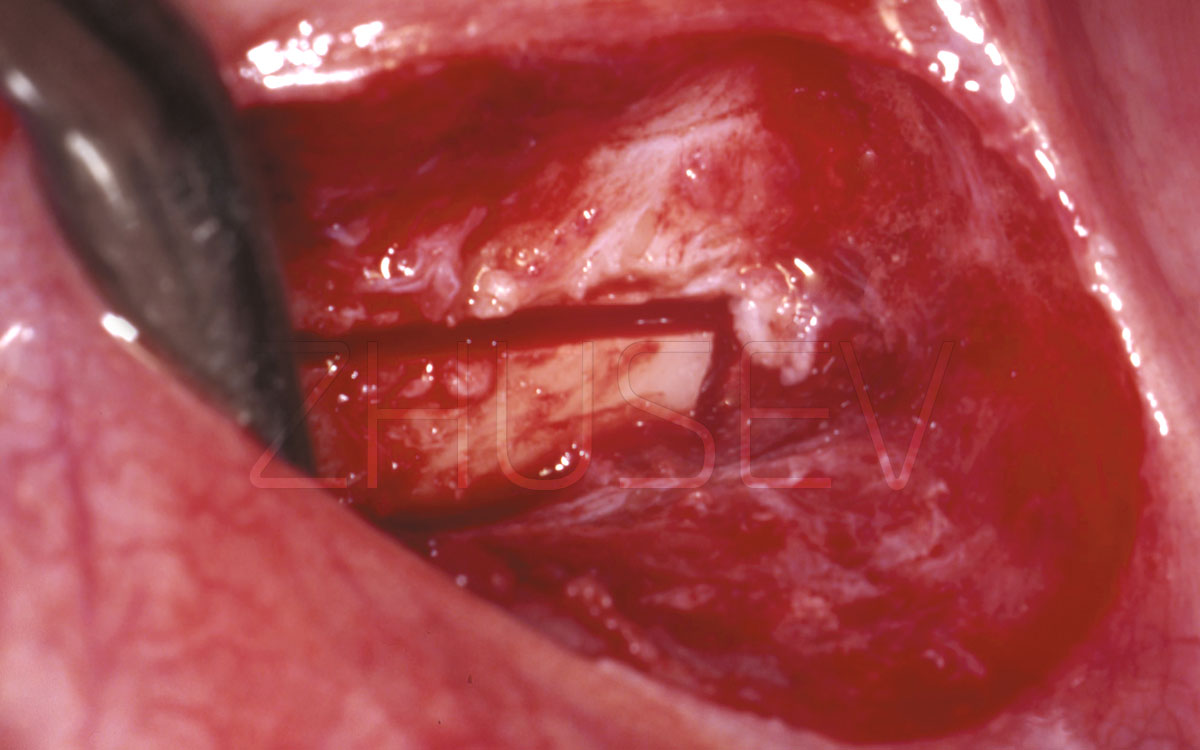
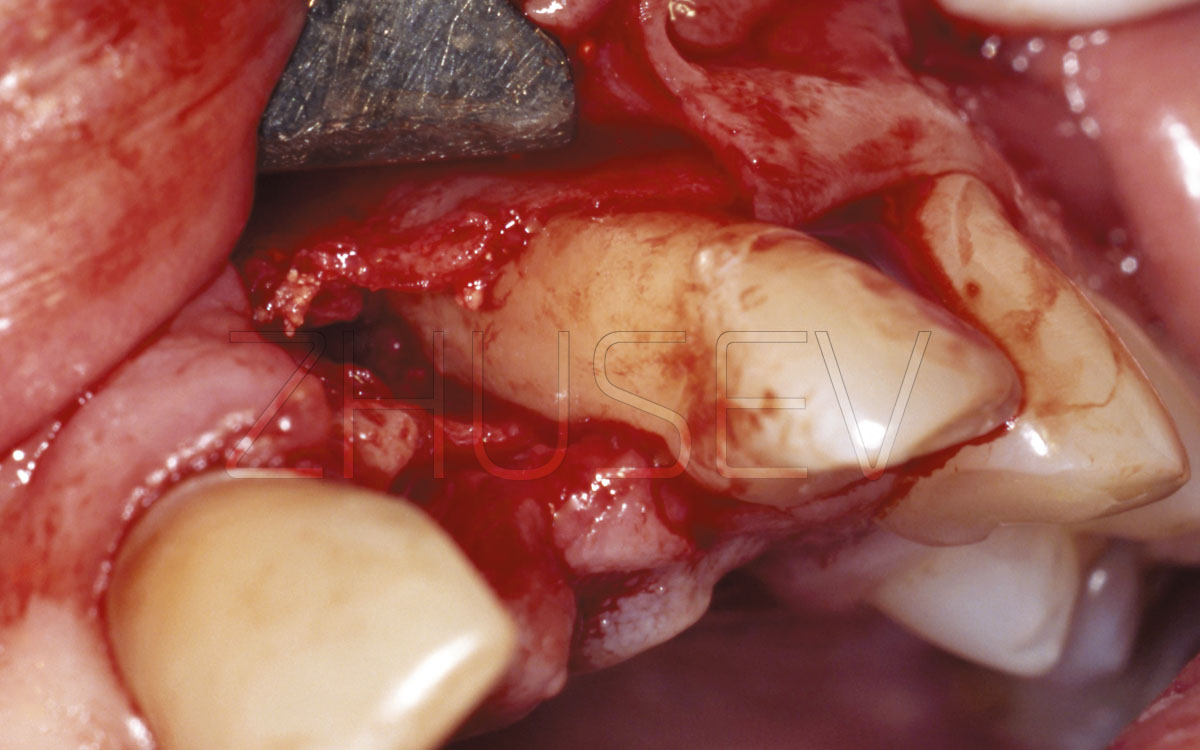
2.8.4-2C
After removing the granulation, the depth of the bone pocket equalled 4/5 of the root’s length. We decided to compensate the defect with CollapAn and a bone block from the mental (mandibular) area.
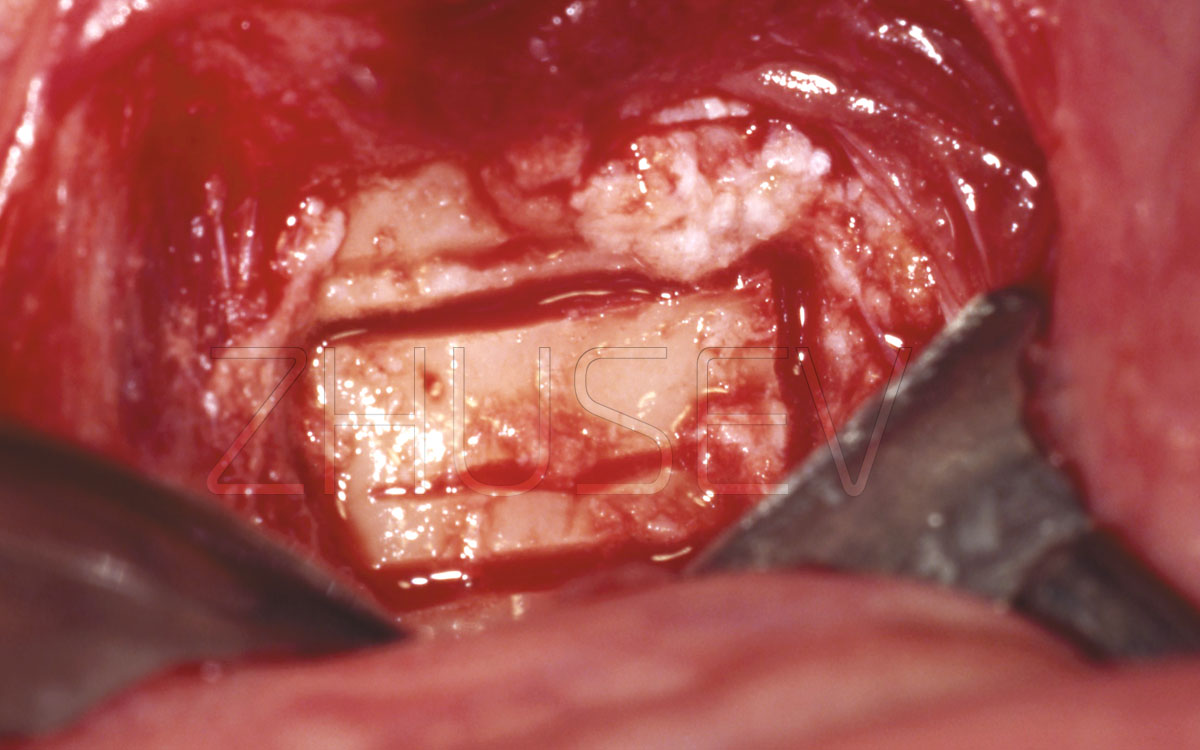
2.8.4-2D
Extraction of a bone block from the mental mandibular area.
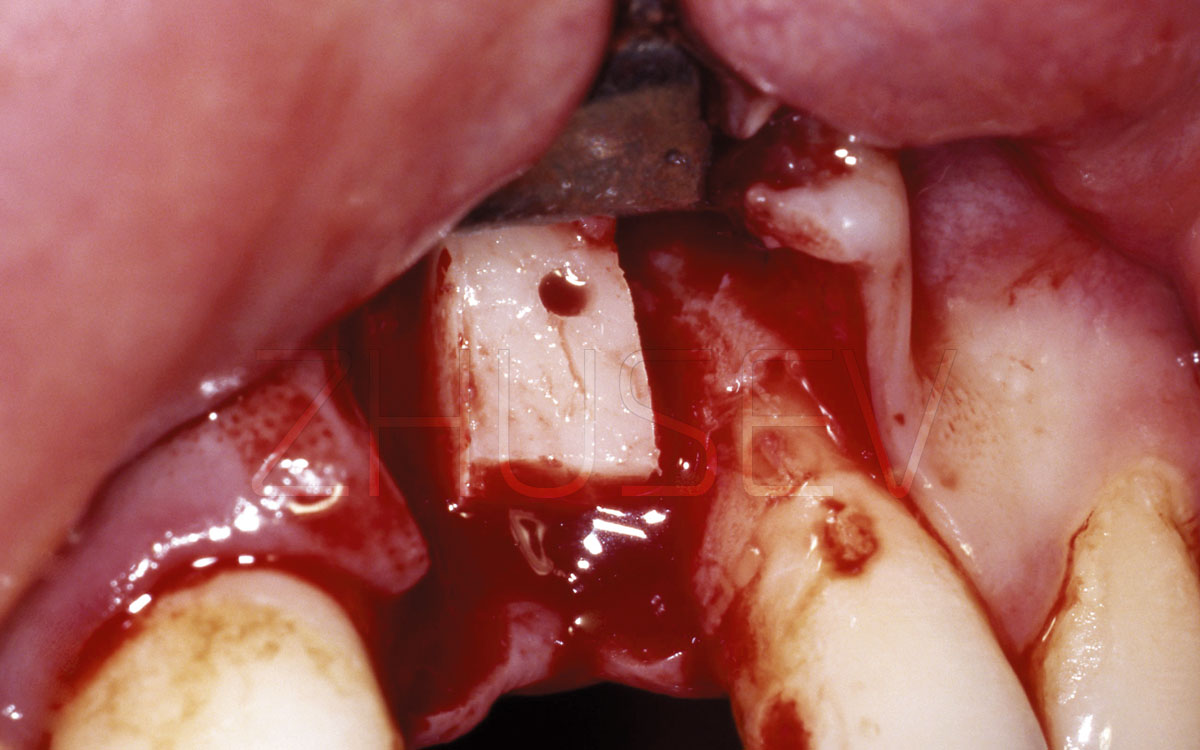
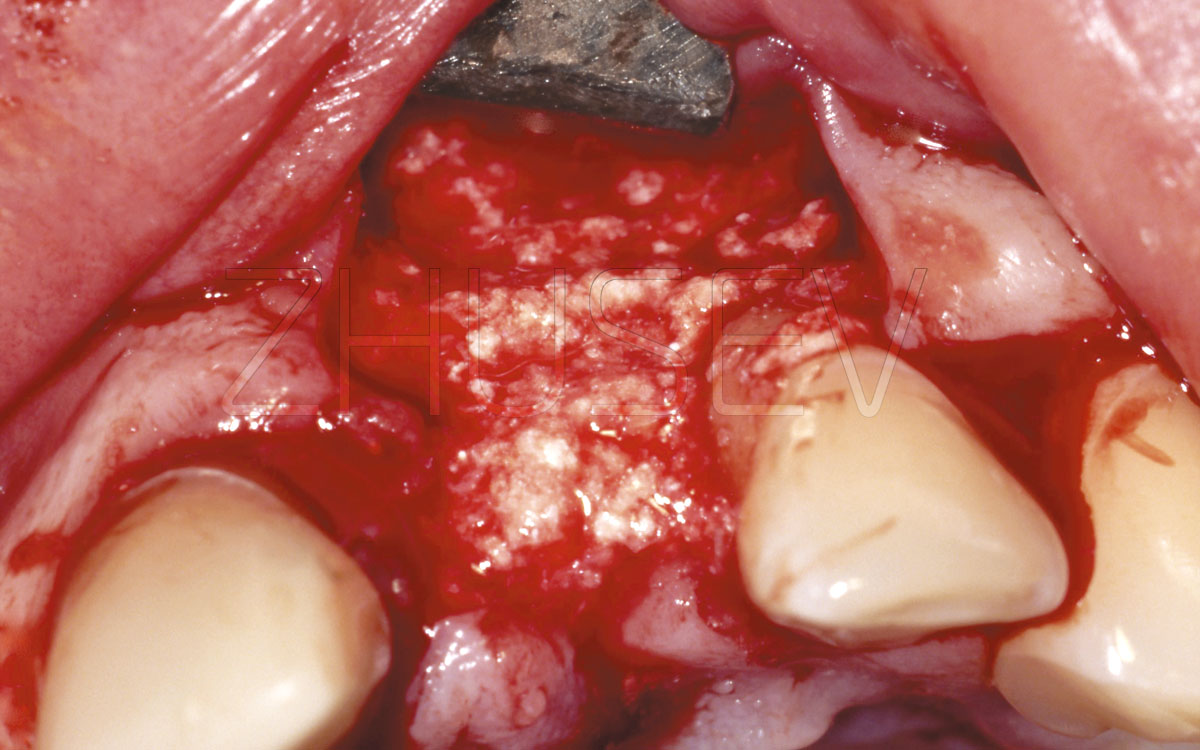
2.8.4-2E
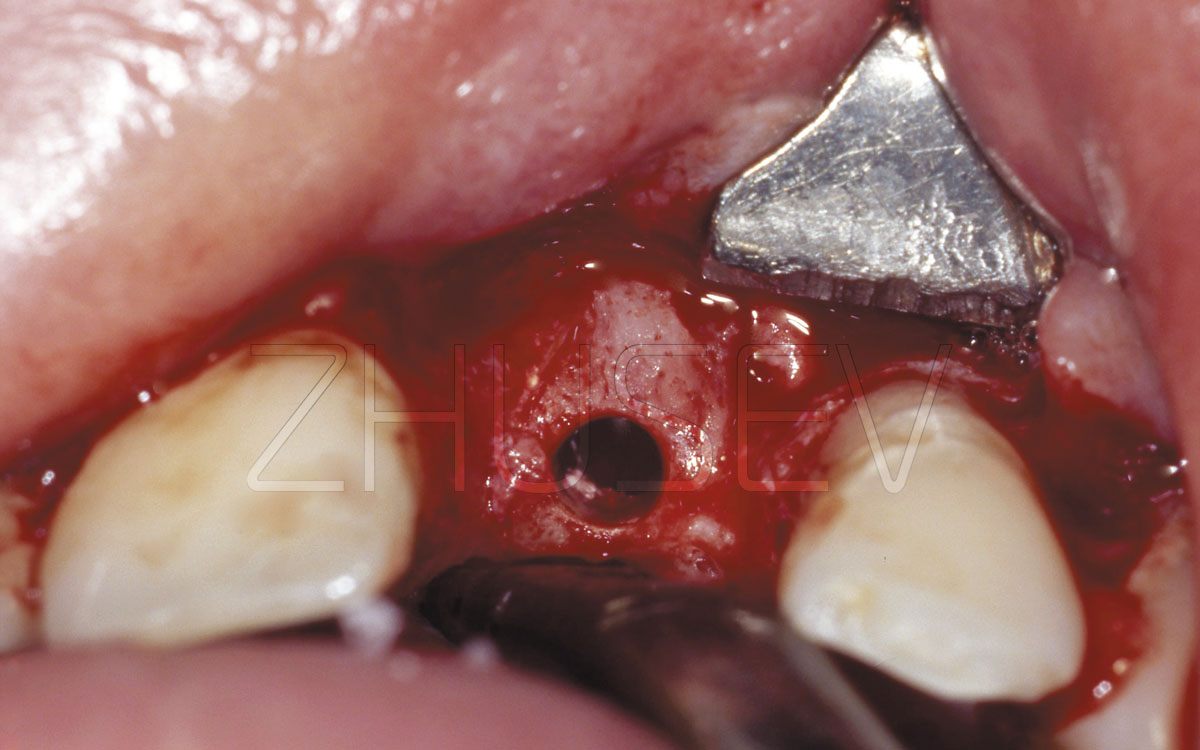
Before the placement of the block, the whole bone pocket of tooth 22 was filled with CollapAn-L. A levelling pad under the block was also made of CollapAn-L.
2.8.4-2F
During the fixation of the bone block, part of the CollapAn levelling pad is squeezed out, filling peripheral defects.
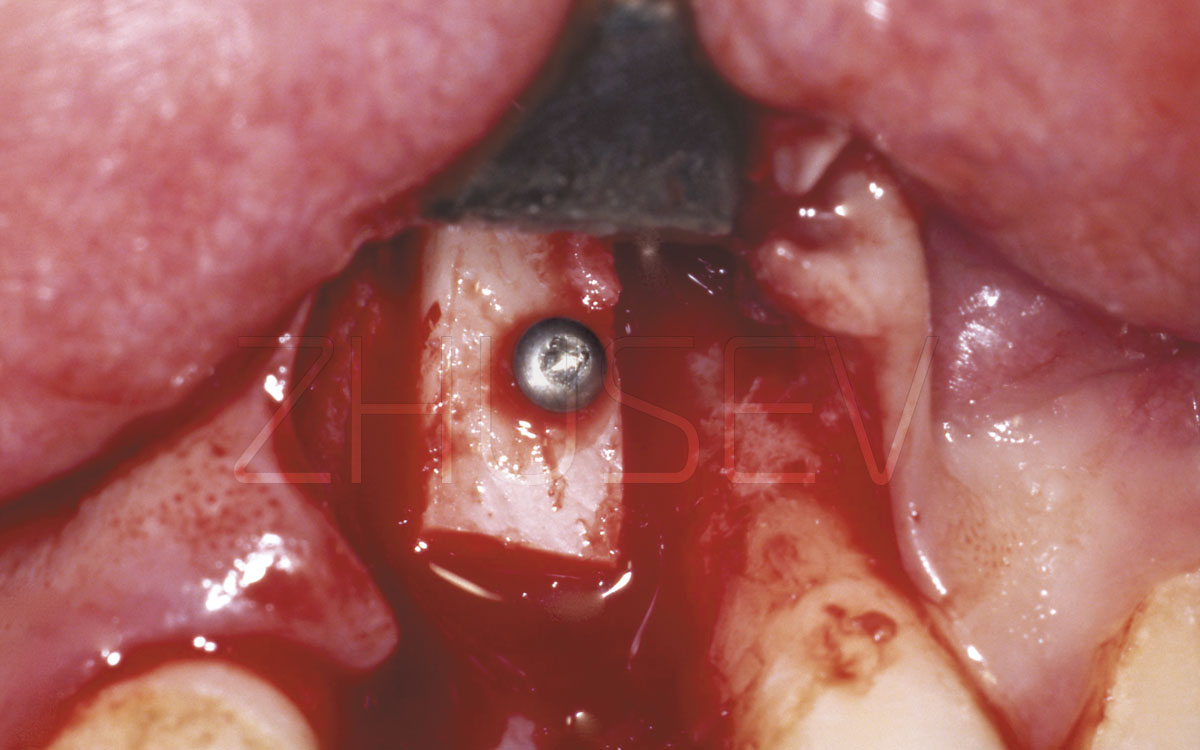
2.8.4-2G
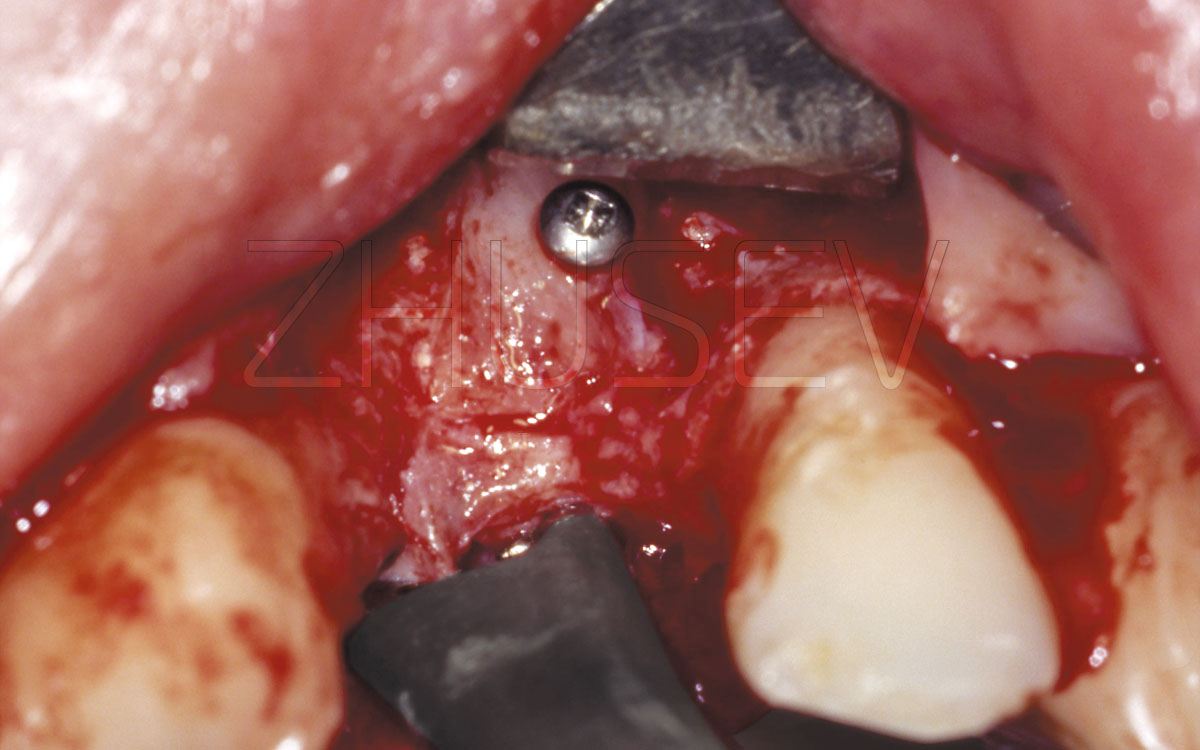
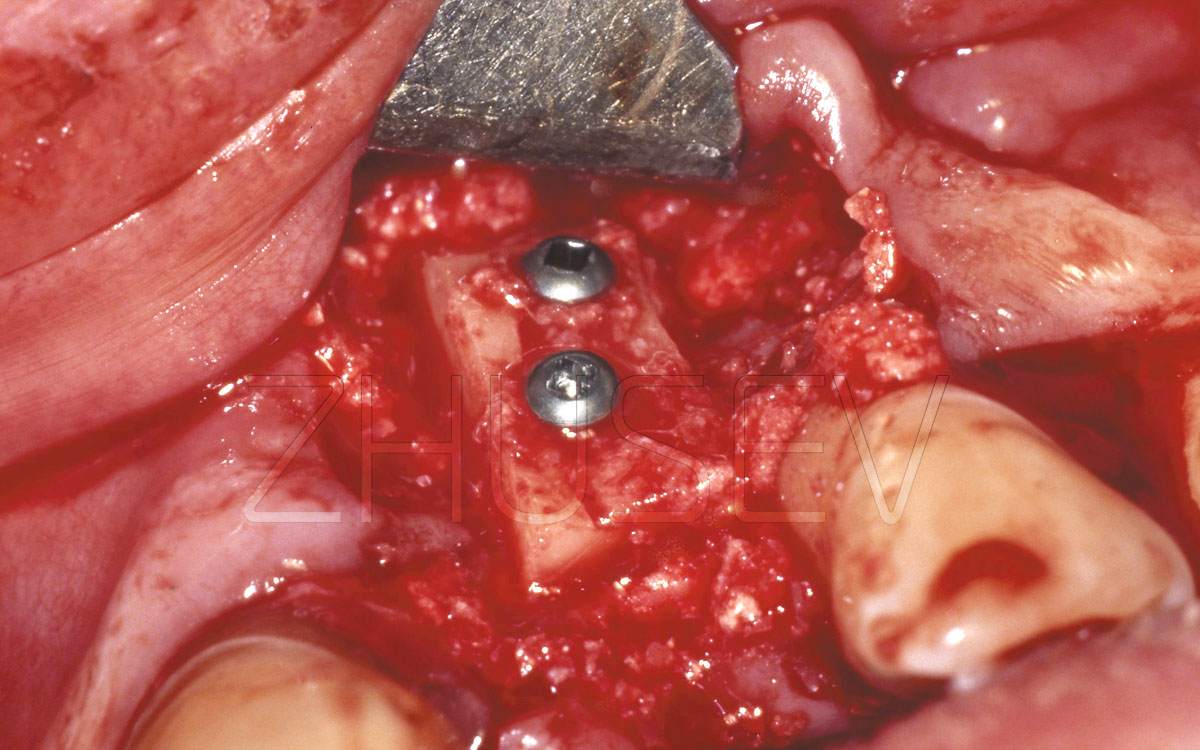
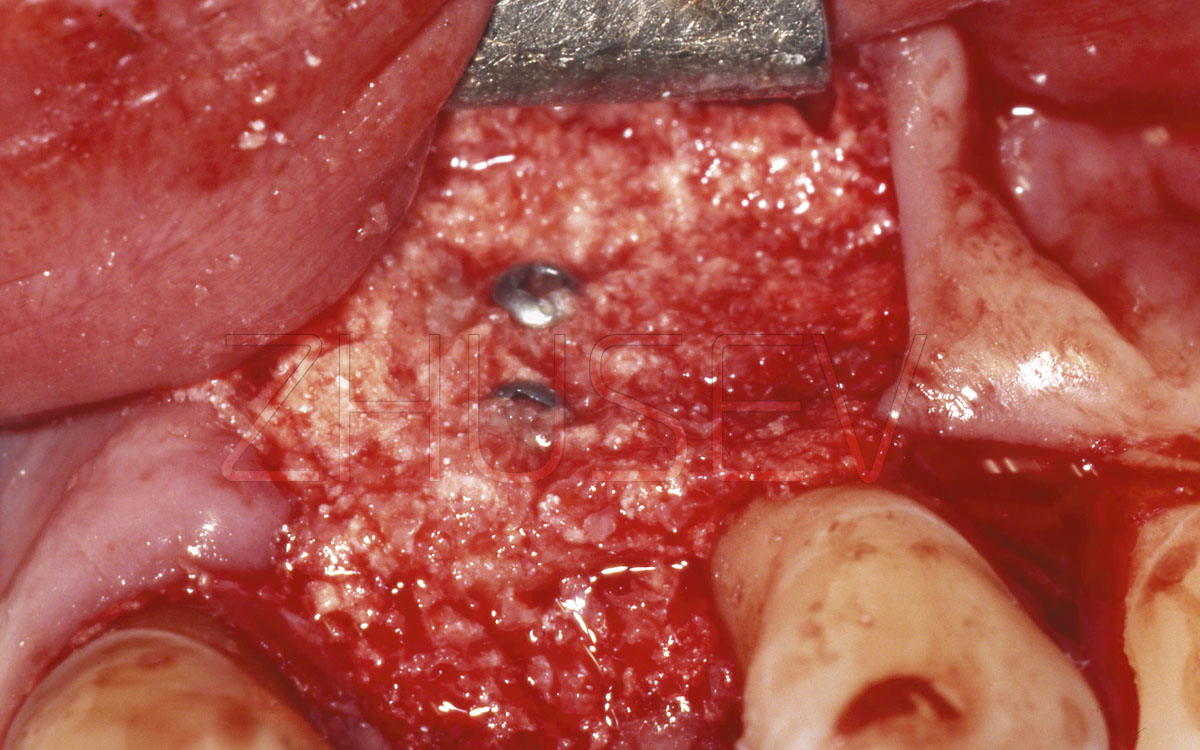
Insignificant mobility of the bone block was found after single-screw fixation, so a second screw was added.
2.8.4-2H
Another layer of CollapAn is added on top of the block. A resorbable membrane (on insert) is added, and the wound is hermetically sutured.