Besides the conventional method of cement-retained fixation, in dental implantology there also is a method of fixation with occlusal screws.
This method provides an opportunity to remove a prosthetic construction at any moment when it is required without destroying it, to perform appropriate procedures, and immediately re-fix it at its place.
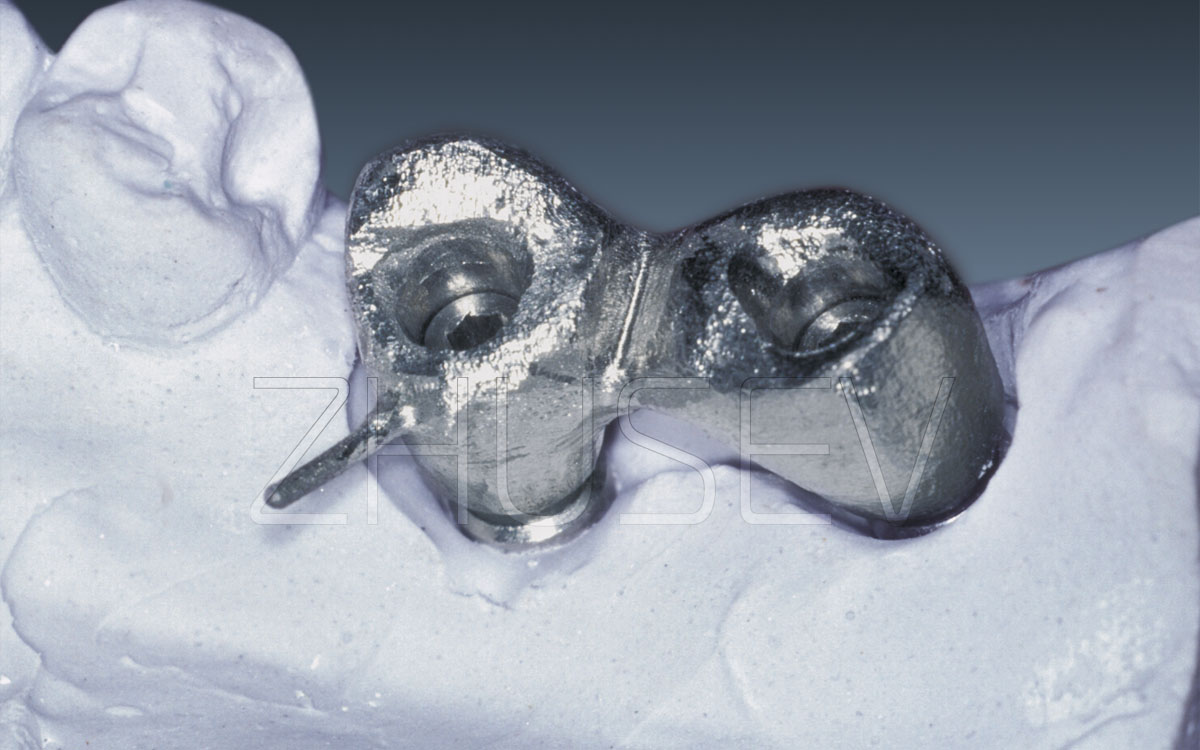
The general sequence of actions of an orthopedic surgeon and a dental technician is the same as in the process of making cement-retained constructions. Its basic feature involves application of special abutments with internal threading for the coronal part’s fixation.
Trying on these constructions is necessary! Moreover, during the try-on, you should always make a reference X-ray and conduct the Sheffield test. When a PFM construction is fully ready and fixed in the mouth, do not cover the fixing screw with a composite material immediately (even if you did everything in keeping with the wrench values). The patient may leave you for 7-10 days. Then invite him to visit your office again, to re-tighten the screws with recommended torque. Covering the screws had better be done only after the third procedure.
So we can apply two methods to fix prosthetic constructions – cement-retained fixation or the use of occlusal screws.
At the start of my career as a practitioner, due to lack of experience and low skills in casting work, I preferred to use cement-retained fixation. Then, when I faced some problems, I followed the words of the Russian general Alexander Suvorov: “When you advance, think about the way to retreat,” and started applying screw-retained fixation more often. Let us try to analyse each technique’s advantages and disadvantages.



Let us start with what is probably the most common technique – cement-retained fixation.
[ + ] Advantages:■ simplicity (a minimum number of specific features, quite full compliance with the work convenient prepared teeth or inlay cores);
■ economic efficiency (no need to buy any additional components and accessories; the only thing you need is fixing cement);
■ high esthetic results;
■ no need of frequent repeated checks of the performed work.
[ – ] Disadvantages:■ difficulty removing the construction when this is required (very often even ultrasound together with a mucotome provide no effect and all crowns have to be cut through);
■ frequent removing of the cement base of the construction when short suprastructures are applied in a limited area;
■ hard adaptation of the construction if it is a single one and based on several convergent implants.
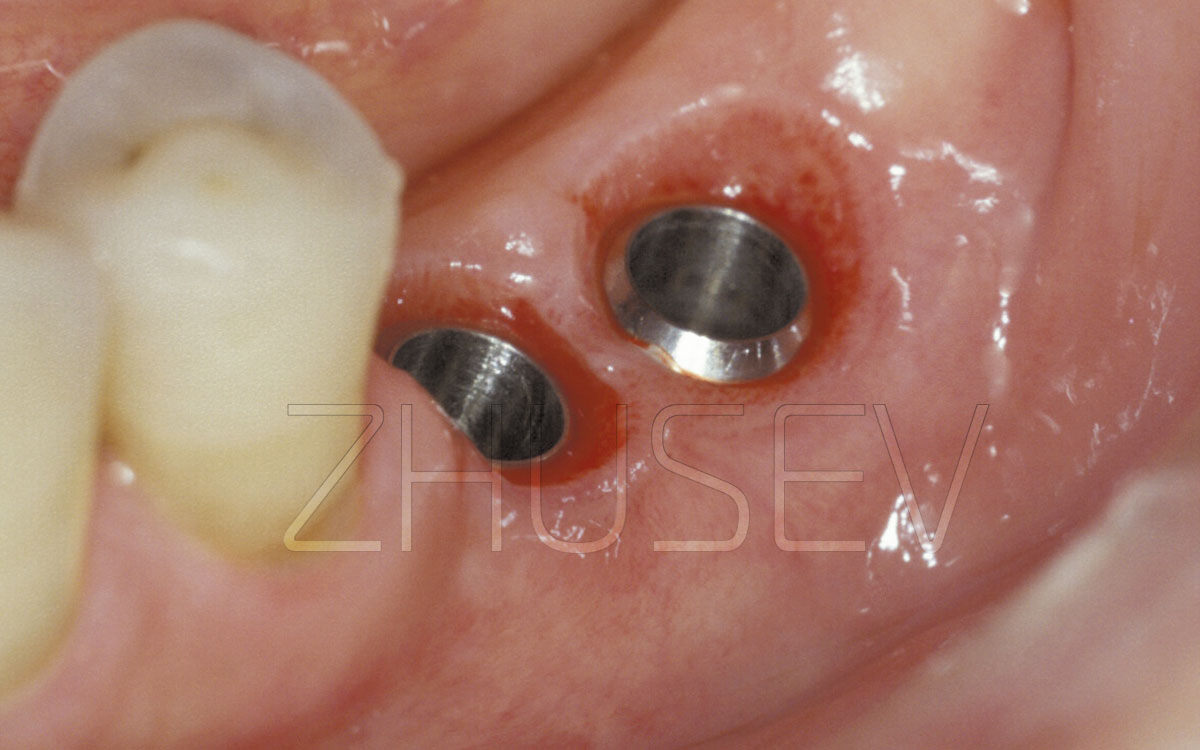
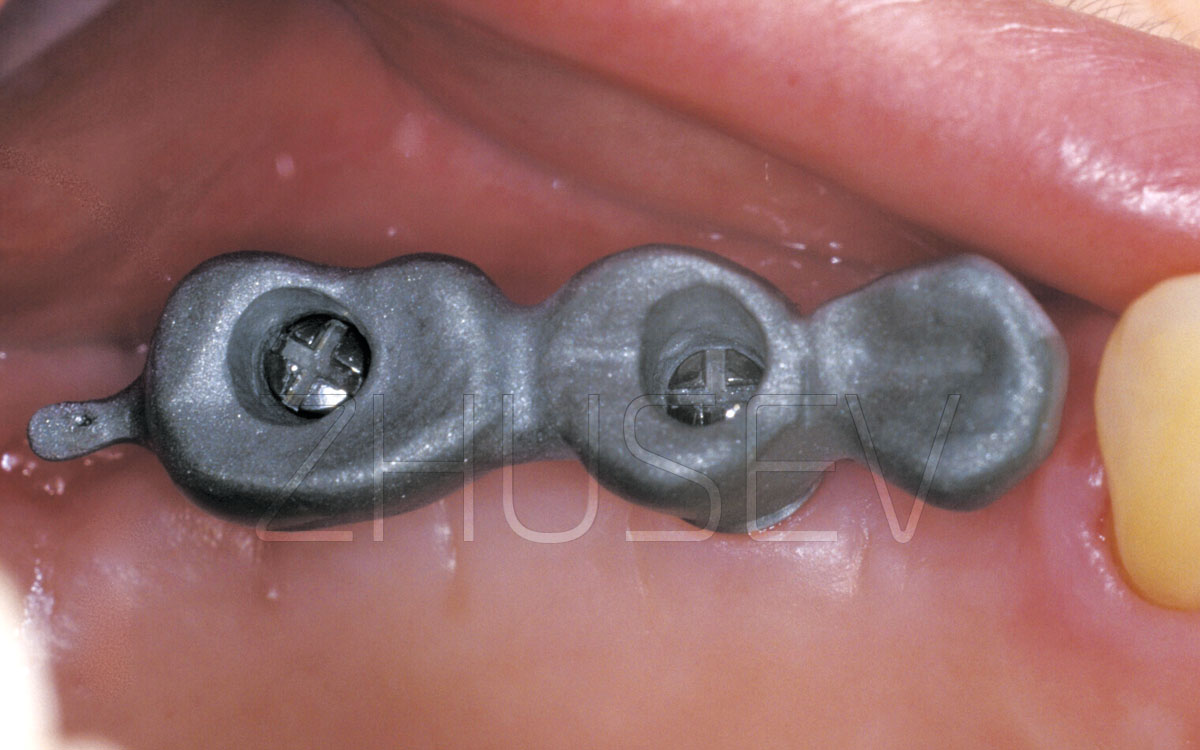
The second widely applied type of orthopedic connection is fixation of constructions with occlusal screws.
[ + ] Advantages:■ the major advantage is the possibility to remove the construction at any moment;
■ reliable fixation even with the shortest and smallest suprastructure;
■ easy fitting and fixing with several implants converging.
[ – ] Disadvantages:■ complexity of manufacture (a very high quality of casting work, high accuracy of the framework processing, covering the screw with composite material, etc. are needed);
■ higher cost (the total cost includes the costs of an abutment, burn-out caps, fixing screw itself, and the cost of covering the screw with composite material);
■ always lower esthetic results compared to cement-retained constructions;
■ necessity to use a torque wrench and X-ray control both during the fitting procedure and a final fixing;
■ control checks, minimum twice a year
WHAT TYPE OF FIXATION TO PREFER?
I think that it is very dangerous to restrict oneself to only one method of fixation!
The main argument for choosing an adequate method of fixation is the specific clinical situation. Let us look at this from the patient’s view. What would each of us like to have as a patient? These are good esthetic and functional results, a fair price for the work and the opportunity to attend the dentist’s office as rare as possible!
Taking this into account, as well as many nuances that I know as a practitioner, I would prefer cement-retained fixation. The only one exception here is a suprastructure’s low clinical height that makes it impossible for any of existing types of cement to retain a prosthetic construction for a long time. Of course, I mean the implant-supported dental constructions with no natural teeth involved. I do mean it. To my mind, this is really a single exception. Even with a number of convergent implants available and the dental technician’s reasonable and correct approach, you may use the method of cement-retained fixation. I am not going to assure you, that a cement-retained fixation should always be preferable. Not at all. Your decision should always be based on individualized approach!
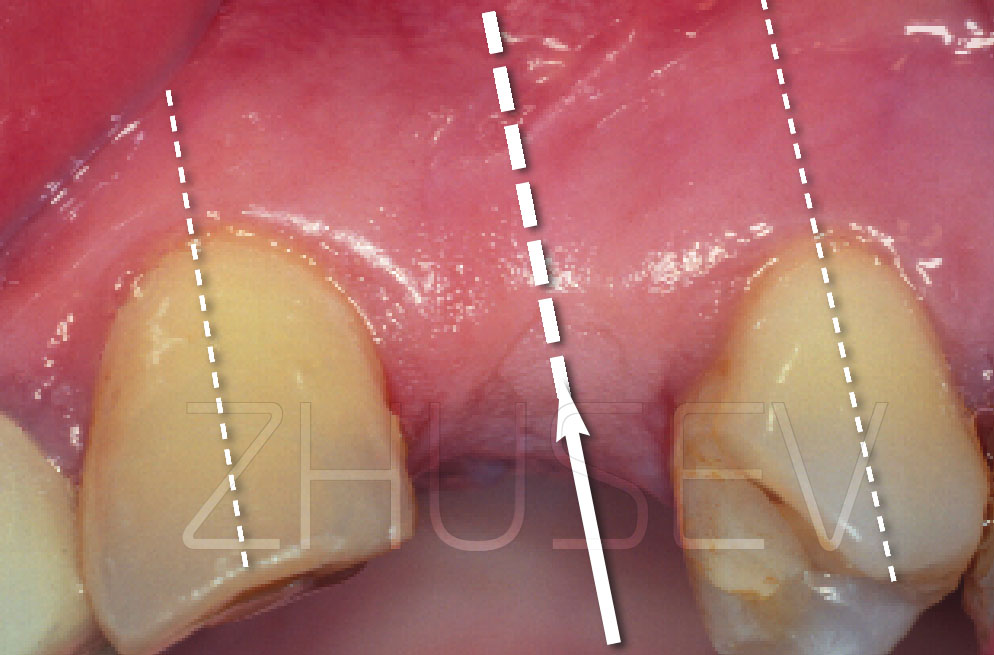
Of course, the best variant is an implant-supported construction with no natural teeth involved! But often, for different reasons (for example, the patient’s financial problems, impossibility to install the required number of implants because of anatomical conditions, etc.) we have to combine both implants and natural teeth. In this case, we need to follow three basic requirements:
Don’t forget the occlusal relationship. Even if you met all these requirements, but ignored the quantity and quality of the occlusal contacts, as well as the type of mastication, the success is not guaranteed! Check the occlusal contacts and relationship several times and be sure tell the patient to come again for control in 3-4 months and in a year! The human body is changing continually, as well as a dentofacial system (and, of course, an occlusion). Remember, that by varying with occlusal contacts only, you can either decrease loading on the prosthetic construction, or create a traumatic ganglion cyst [occlusion], that invariably will cause unwanted consequences.